Medical publication policies and guidelines offer a framework for best practices, but there may be situations when more than one approach seems reasonable. The primary purpose of “What Would You Do?” is to explore examples of such situations. With the limited information provided to interpret the scenarios, you may find yourself agreeing with one, more than one, or none of the proposed actions. And that’s the point ‒ you should debate, contemplate, and communicate (with a comment) before selecting your “best” answer.
Now let’s find out how you responded and read through some commentary (for context only; not meant to be comprehensive) to the below scenario:
A medical writer worked with authors to develop a congress abstract for a Phase 2 clinical study. Two days before submission, the lead author requests an additional ‘medical narrative’ statement to be added detailing the management steps and time to resolution of an adverse event seen in one patient.
{kind=link}
A. It is too late to add anything to the abstract, and you are already at the character limit. Go ahead and submit the abstract since you already received the lead author’s approval email.
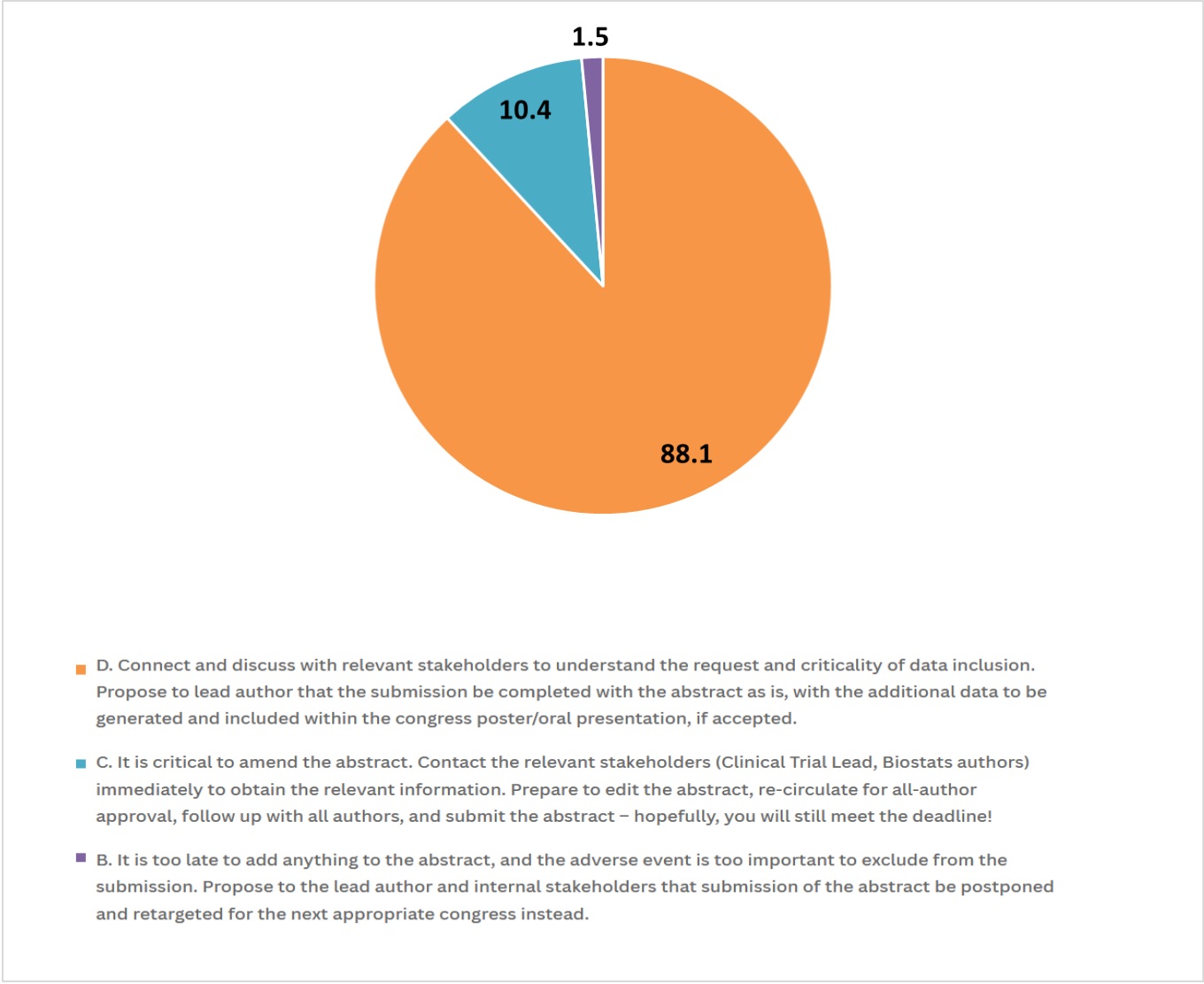
B. It is too late to add anything to the abstract, and the adverse event is too important to exclude from the submission. Propose to the lead author and internal stakeholders that submission of the abstract be postponed and retargeted for the next appropriate congress instead.
C. It is critical to amend the abstract. Contact the relevant stakeholders (Clinical Trial Lead, Biostats authors) immediately to obtain the relevant information. Prepare to edit the abstract, re-circulate for all-author approval, follow up with all authors, and submit the abstract – hopefully, you will still meet the deadline!
D. Connect and discuss with relevant stakeholders to understand the request and criticality of data inclusion. Propose to lead author that the submission be completed with the abstract as is, with the additional data to be generated and included within the congress poster/oral presentation, if accepted.

A total of 67 people replied to this poll.
For a typical clinical development program evaluating a non-orphan disease, we can expect a phase 2 study to include as few as 25-50 patients or as many as 100-300 patients. With sample sizes of this range, one patient accounts for a small proportion of the overall dataset. Abstracts usually provide an overview of the efficacy and safety results, rarely going into a lot of detail about an individual patient; it is not a case study and the outcomes for a single patient should not be overstated. For these reasons, Option C would generally not be pursued.
As for Option B, depending on how many authors are involved and how well communications are managed, it is possible to update an abstract in 2 days, and investigators and sponsors generally do not want to delay the publication of data. And given that it is the lead author who is asking for the update to the abstract, the team needs to circle back on the previous approval because there is documentation that the current version is no longer acceptable, so we can strike Option A.
This leaves us with Option D, which is the recommended approach. To help with discussions, it would be good to understand why the lead author wishes to single out the patient; was the patient someone the lead author personally treated in the trial or perhaps the narrative supports the personal research interests of the lead author? All authors and relevant stakeholders should be involved in objective, thoughtful scientific exchange to develop the best possible abstract that represents the totality of the results from the trial and align on how to best communicate different aspects of the results. If escalation is needed to resolve the issue, refer to company policies or publication steering committee charters on the appropriate next steps to take.
Eric Y. Wong, PhD, MBA, ISMPP CMPPTM, Johnson & Johnson Innovative Medicine
This article was prepared by the author in his personal capacity. The opinions expressed within are the author’s own and do not necessarily reflect the views of Johnson & Johnson Innovative Medicine.