
Yvonne E. Yarker, PhD, ISMPP CMPP™, Medicite LLC, Yardley, PA, USA
On September 8, 2018, the New York Times, in collaboration with ProPublica, a nonprofit investigative journalism group, reported that a leading oncologist at Memorial Sloan Kettering Cancer Center (MSKCC) in New York had failed to report financial relationships with multiple pharmaceutical companies in his publications in prestigious medical journals.1,2 Dr. José Baselga was the chief medical officer at MSKCC, an internationally renowned researcher in molecular targeted therapies, and the lead author of several key clinical trials of targeted therapies in breast cancer research.3-6 Now, in a more recent report published on December 8, 2018, by the New York Times and ProPublica, the accusations of failure to disclose pharmaceutical industry funding in journal publications have expanded to include several more leading clinicians, including Dr. Howard Burris III, incoming President of the American Society of Clinical Oncology (ASCO).7
A search of PubMed shows that Dr. Baselga was the first author of 26 medical publications over the last 10 years, and a coauthor of hundreds more. He has published in prestigious general medical journals, such as the Journal of the American Medical Association (JAMA), The Lancet, and The New England Journal of Medicine (NEJM), as well as major international oncology journals, such as Annals of Oncology and the Journal of Clinical Oncology. He is also a past President of major international oncology organizations, served as an editor for several journals, and has received accolades from leading institutions and societies for his research contributions.
Why Is Failure to Disclose Important?
Given the reputation and experience of Dr. Baselga and the other individuals named by the New York Times and ProPublica, reports of their failure to disclose financial relationships and potential conflicts of interest (COIs) when submitting their work for publication is disturbing. In Dr. Baselga’s case, according to ProPublica, he did not disclose financial relationships with pharmaceutical and biotech companies in 60% of almost 180 publications since 2013, and in 87% of publications in 2017,1,2 based on a review of the US Centers for Medicare & Medicaid Services (CMS) Open Payments portal (a national program that collects and publishes financial payments made by drug and medical device companies to physicians), which shows that annual payments to Dr. Baselga from industry sources ranged from several thousand US dollars to over two million US dollars over the last five years.8 Notably, these payments are listed as “general payments,” so it is not clear whether they were made to him personally or to his institution.
In response to the report, Dr. Baselga indicated that his industry relationships were well known (and are publicly available on the CMS website) and he would correct his disclosure statements for some publications, but that he believed that financial disclosures in other cases were not required because of the nature of the publications. Several statements from Dr. Baselga to correct his disclosure omissions have now been published in JAMA journals,9-11 and it is likely that similar statements will appear in other journals. These disclosures include his position on the boards of directors of several pharmaceutical and biotech companies, serving on scientific advisory boards, receiving consultancy fees, owning company stock, and being involved in several patents.
The personal consequences of this news have been significant for Dr. Baselga: he resigned from MSKCC and from the Board of Directors of Bristol-Myers Squibb.2,12 An internet search revealed that reactions to the ProPublica and New York Times report of September 8 and to his subsequent resignations and disclosure statements have been mixed, ranging from outrage at his perceived unethical practices in failing to disclose significant financial relationships to concerns that he has been condemned and his reputation tarnished for something that is likely a common failing among researchers and authors, whether inadvertent or deliberate. Although his own integrity has been questioned, some wonder whether his disclosure omissions really affect the integrity of his research. Similar reactions have been posted to the most recent report of December 8, ranging from demands to charge such researchers with misconduct to calls for a clearer and more simplified system of reporting disclosures to journals.7
Increasing Focus on Disclosures of Conflicts of Interest
Over the last 10 years, according to PubMed, the number of research and commentary articles in the biomedical literature with “conflict(s) of interest” in the title has increased from five in 2008 to 145 through November 2018, a number that is likely to increase by the end of the year; articles relating to issues raised by Dr. Baselga’s situation have already appeared in medical journals.13,14 A research article published in JAMA this year reported that in 77% of over 1,000 biomedical journal articles, either the authors reported that they had no COIs or they didn’t report COIs at all, certainly a cause for concern.15
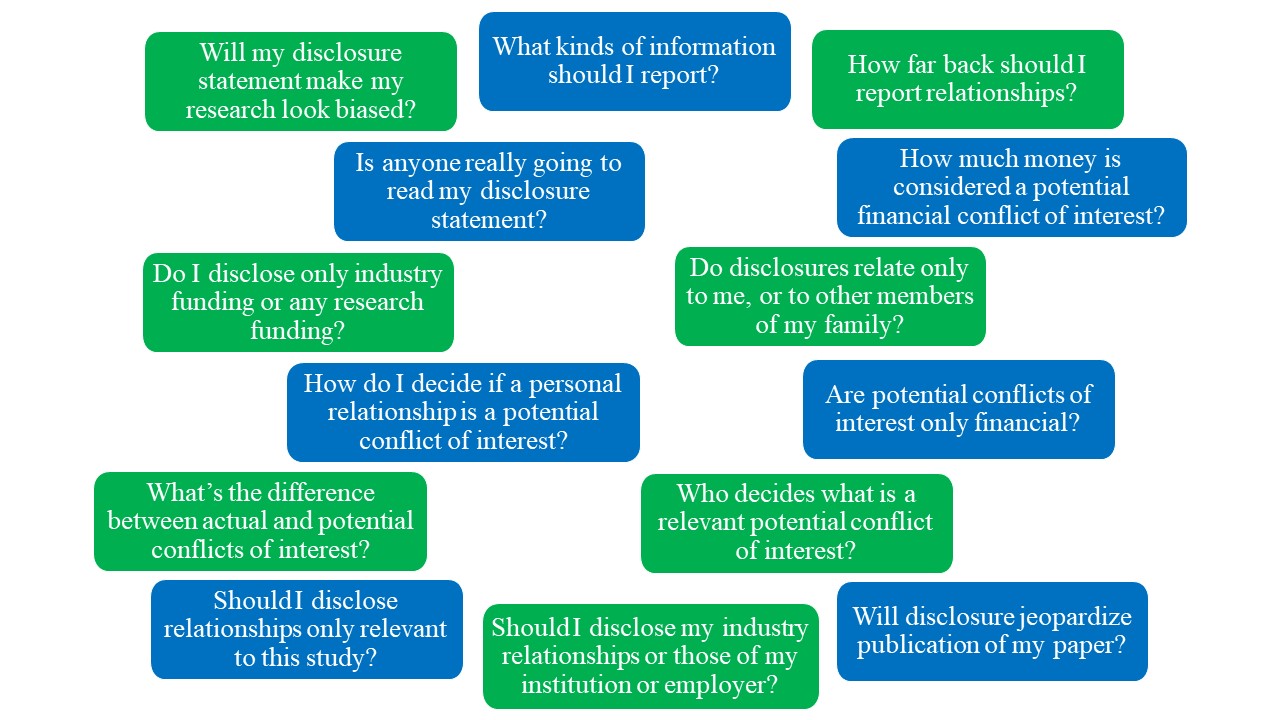
A fundamental issue is that the notions of disclosure and COI are contentious and confusing themselves – what is the definition of a potential COI, does disclosure relate to the individual or also to his or her employer, what types of disclosures are relevant, how far back should such disclosures be reported, and what constitutes transparency (see Figure 1 below)?
Figure 1. Questions about COIs in Biomedical Publications
{kind=link}

Concern over relationships between physicians, teaching hospitals, and pharmaceutical, medical device, and biotech companies led to the 2010 Physician Payments Sunshine Act in the US, which mandated transparency in reporting these financial relationships. The statutory requirement is fulfilled by the CMS Open Payments Program. Nonetheless, clear and consistent guidance from biomedical journals to their authors on appropriate disclosures is lacking. Some efforts to create central repositories for disclosures are in progress, such as Convey, a centralized repository to capture disclosures, which was developed in collaboration between the NEJM and the Association of American Medical Colleges.16 Another initiative trying to standardize information requirements relating to research funding and publication is the Consortia Advancing Standards in Research Administration Information (CASRAI), although it does not currently have specific recommendations about disclosures.
Guidance for Authors on Disclosures and Conflicts of Interest
The International Committee of Medical Journal Editors (ICMJE), the leading source of guidance for biomedical journal editors, states that “A conflict of interest exists when professional judgment concerning a primary interest (such as patients’ welfare or the validity of research) may be influenced by a secondary interest (such as financial gain). Perceptions of conflict of interest are as important as actual conflicts of interest.” In 2009, ICMJE published a standardized and interactive form for authors to disclose potential COIs, which was updated in 2010.17 The World Association of Medical Editors (WAME) has a 2009 policy statement that provides guidance on COI policies for medical journals, but does not provide practical tools for authors wishing to report their disclosures.18 The EQUATOR Network, a repository of reporting guidelines relevant to the biomedical literature, lists six reporting guidelines relating to COI, of which only two provide practical checklists or forms: the ICMJE COI form and a checklist specific to financial COIs.19 The Good Publication Practice (GPP3) guidelines generally propose using the ICMJE form and reporting relevant relationships over a three-year time period.20
Individual biomedical journal requirements for disclosures vary considerably. The ICMJE form has been adopted by many leading journals but has been adapted or revised in some cases. Table 1 below shows key disclosure and COI guidance from top general medical journals and oncology journals and demonstrates the complexity and variability of their guidance for authors.
Table 1. Disclosure and COI Statements in Key Biomedical and Oncology Journals
| Journal | Sources | Key Disclosure or COI Reporting Statements |
| JAMA | https://jamanetwork.com/journals/jama/pages/instructions-for-authors#SecConflictsofInterestandFinancialDisclosures | Provide detailed information about all relevant financial interests, activities, relationships, and affiliations including, but not limited to, employment, affiliation, funding/grants received or pending, consultancies, honoraria or payment, speakers’ bureaus, stock ownership or options, expert testimony, royalties, donation of medical equipment, or patents planned, pending, or issued.
If uncertain about what constitutes a relevant financial interest or relationship, contact the editorial office. Downloadable Author form, which includes questions from the ICMJE COI form. |
| Lancet | https://www.thelancet.com/pb/assets/raw/Lancet/authors/tl-info-for-authors.pdf | A COI exists when professional judgement concerning a primary interest (such as validity of research) may be influenced by a secondary interest (such as financial gain). Financial relationships are easily identifiable, but conflicts can also occur because of personal relationships or rivalries, academic competition, or intellectual beliefs. A conflict can be actual or potential, and full disclosure is the safest course. Failure to disclose COIs might lead to an erratum or even retraction.
All submissions must include disclosure of all relationships that could be potential or actual COIs. The Editor may use such information as a basis for editorial decisions and will publish such disclosures if they are believed to be important to readers in judging the manuscript. Downloadable ICMJE COI form. |
| NEJM | https://www.nejm.org/doi/pdf/10.1056/NEJMe020074
https://www.nejm.org/pb-assets/pdfs/ICMJEDisclosureForm0521101RE-1502468766397.pdf |
For original articles, discloses sponsorship of the studies and relevant financial information about the authors. During the editorial process, authors are asked for details of their financial relationships with biomedical companies, such as consulting fees, service on advisory boards, ownership of equity (or options), patent royalties, honorariums for lectures, expert testimony fees, and research grants. We report all relevant financial relationships; if an author has reported no relevant financial relationships, there is no statement.
Downloadable ICMJE COI form and example of a completed COI form. |
| Ann Oncol | https://academic.oup.com/annonc/pages/General_Instructions
https://academic.oup.com/journals/pages/authors/ethics#conflict https://academic.oup.com/journals/pages/authors/authors_faqs/conflicts_of_interest |
Any financial interests or connections, direct or indirect, or other situations that might raise the question of bias in the work reported or the conclusions, implications or opinions stated – including pertinent commercial or other sources of funding for individual authors or for their departments or organizations, personal relationships, or direct academic competition – should be disclosed.
Report all sources of research funding, including direct and indirect financial support, supply of equipment, or materials (including specialist statistical or writing assistance). Report any relevant financial and non-financial interests and relationships that might be considered likely to affect the interpretation of their findings or that editors, reviewers, or readers might reasonably wish to know. These might include, but are not limited to, patent or stock ownership, membership on a company’s board of directors, membership of an advisory board or committee for a company, consultancy for a company, or receipt of speaker’s fees from a company. When considering whether to declare a COI or connection, ask this question: is there any arrangement that would compromise the perception of your impartiality or that of your co-authors if it was to emerge after publication and you had not declared it? If there are none, the disclosure should say: ‘The authors have declared no conflicts of interest.’ If one or more authors have a conflict to disclose, further to that statement, there should be an additional statement for the remaining authors who do not have any COI to declare. |
| J Clin Oncol | http://ascopubs.org/jco/site/ifc/journal-policies.xhtml
http://ascopubs.org/pb-assets/pdfs/JCO_required_author_info-1474312265177.pdf |
Requires general or full disclosure as opposed to activity-specific disclosure. Answer each question to reflect all your financial relationships with companies over the past 2 years, regardless of whether any relationships with a company is specifically related to the subject of a manuscript. All relationships including research funding must be disclosed, even if funding is paid to your institution. Failure to provide complete and accurate disclosure is a violation of ASCO policies and could result in errata, retraction, or restrictions on future publication with ASCO. Double check your disclosure against other sources to identify publicly reported interactions with companies that you may have omitted. Downloadable form for disclosure and authorship contributions. |
What Is the Role of the Medical Publication Professional?
The medical publication professional is often required to collect disclosure information from authors during the development and submission of presentations to congresses and manuscripts to journals. As such, they are likely to receive questions from authors about what to disclose and need to encourage authors to provide their information in a timely manner. Some journal editors have stated that they cannot verify every author disclosure statement, and similarly, medical publication professionals are not responsible for the accuracy or completeness of author disclosure statements. However, they can assist authors in providing appropriate disclosures and in streamlining a sometimes onerous process. Some suggestions to facilitate the collection of appropriate disclosures in an efficient manner are listed in Table 2 below.
Table 2: Upfront Preparation and Author Disclosure Support Activities for Medical Publication Professionals
| Upfront Preparation | Author Disclosure Support |
|
|
The continuing scrutiny of relationships between biomedical researchers and industry has led to a surge in disclosure requirements by biomedical journals and congresses, and there is much debate in the biomedical literature about the need for transparency. Yet, guidance for authors is confusing, ambiguous, and inconsistent. Until such requirements are clearly defined, authors will continue to be at risk for exposure and sanction over incomplete disclosures, whether because of carelessness, a lack of understanding of what constitutes appropriate disclosure, or intentional omission. In the meantime, medical publication professionals can provide valuable support and guidance to authors to help them submit accurate and comprehensive disclosure statements.
Disclosures: The author is a past Chair of the ISMPP Board of Trustees and a member of ASCO. No funding was received for the development of this article.
References
- Ornstein C, Thomas K. Top cancer researcher fails to disclose corporate financial ties in major research journals. New York Times; September 8, 2018.
- Ornstein C, Thomas K. Top official at Memorial Sloan Kettering resigns after failing to disclose industry ties. ProPublica; September 13, 2018.
- Baselga J, Swain SM. CLEOPATRA: a phase III evaluation of pertuzumab and trastuzumab for HER2-positive metastatic breast cancer. Clin Breast Cancer. 2010;10(6):489-491.
- Baselga J, Bradbury I, Eidtmann H, et al. Lapatinib with trastuzumab for HER2-positive early breast cancer (NeoALTTO): a randomised, open-label, multicentre, phase 3 trial. Lancet. 2012;379(9816):633-640.
- Baselga J, Zamagni C, Gomez P, et al. RESILIENCE: Phase III randomized, double-blind trial comparing sorafenib with capecitabine versus placebo with capecitabine in locally advanced or metastatic HER2-negative breast cancer. Clin Breast Cancer. 2017;17(8):585-594.e584.
- Baselga J, Campone M, Piccart M, et al. Everolimus in postmenopausal hormone-receptor-positive advanced breast cancer. N Engl J Med. 2012;366(6):520-529.
- Ornstein C, Thomas K. What these medical journals don’t reveal: top doctors’ ties to industry. New York Times; December 8, 2018.
- Jose M. Baselga. Centers for Medicare & Medicaid Services (CMS) 2018.
- Baselga J. Failure to accurately disclose conflicts of interest in articles published in JAMA Oncology. JAMA Oncol. 2018.
- Baselga J. Failure to disclose conflict of interest in article published in JAMA on detection of cancer-related genes. JAMA. 2018.
- Baselga J. Failure to accurately disclose conflicts of interest in article published in JAMA Otolaryngology-Head & Neck Surgery. JAMA Otolaryngol Head Neck Surg. 2018.
- Bristol-Myers Squibb Statement on Resignation of Dr. José Baselga [press release]. Bristol-Myers Squibb, 14 September, 2018.
- Bauchner H, Fontanarosa PB, Flanagin A. Conflicts of interests, authors, and journals: New challenges for a persistent problem. JAMA. 2018.
- Chabner BA, Bates SE. Conflict of interest: an ethical firestorm with consequences for cancer research. Oncologist. 2018.
- Grundy Q, Dunn AG, Bourgeois FT, Coiera E, Bero L. Prevalence of disclosed conflicts of interest in biomedical research and associations with journal impact factors and altmetric scores. JAMA. 2018;319(4):408-409.
- Drazen JM. For full disclosure in medicine. New York Times; September 30, 2018.
- Drazen JM, de Leeuw PW, Laine C, et al. Toward more uniform conflict disclosures–the updated ICMJE conflict of interest reporting form. N Engl J Med. 2010;363(2):188-189.
- Ferris LE, Fletcher RH. Conflict of interest in peer-reviewed medical journals: the World Association of Medical Editors (WAME) position on a challenging problem. Cardiovasc Diagn Ther. 2012;2(3):188-191.
- Rochon PA, Hoey J, Chan AW, et al. Financial conflicts of interest checklist 2010 for clinical research studies. Open Med. 2010;4(1):e69-91.
- Battisti WP, Wager E, Baltzer L, et al. Good publication practice for communicating company-sponsored medical research: GPP3. Ann Intern Med. 2015;163(6):461-464.