
Meredith Rogers, MS, ISMPP CMPPTM, The Lockwood Group, Stamford, CT, USA
This article is part of the Medical Publications 101 article series, which serves as an introduction to various topics that are relevant to medical publication professionals.
The first reference to a clinical trial can be found in the Bible. In that trial, conducted by King Nebuchadnezzar II (605-562 BC), children fed a strict diet of meat and wine were compared to children fed pulses (eg, beans, peas, lentils) and followed for 3 years (by the way, the children on the meat and wine diet were deemed healthier).
Clinical trials, defined as any interventional study involving humans, are critical to advancement of medical knowledge. While not all trials are created equal, the goal of every trial is to provide maximum information with the least risk to study participants. In general, a clinical trial involves providing an active intervention, whether that be a drug, device, surgical procedure, or behavioral change, to investigate the effect of a treatment, preventive technique, or diagnostic modality.
Phases of Clinical Trials
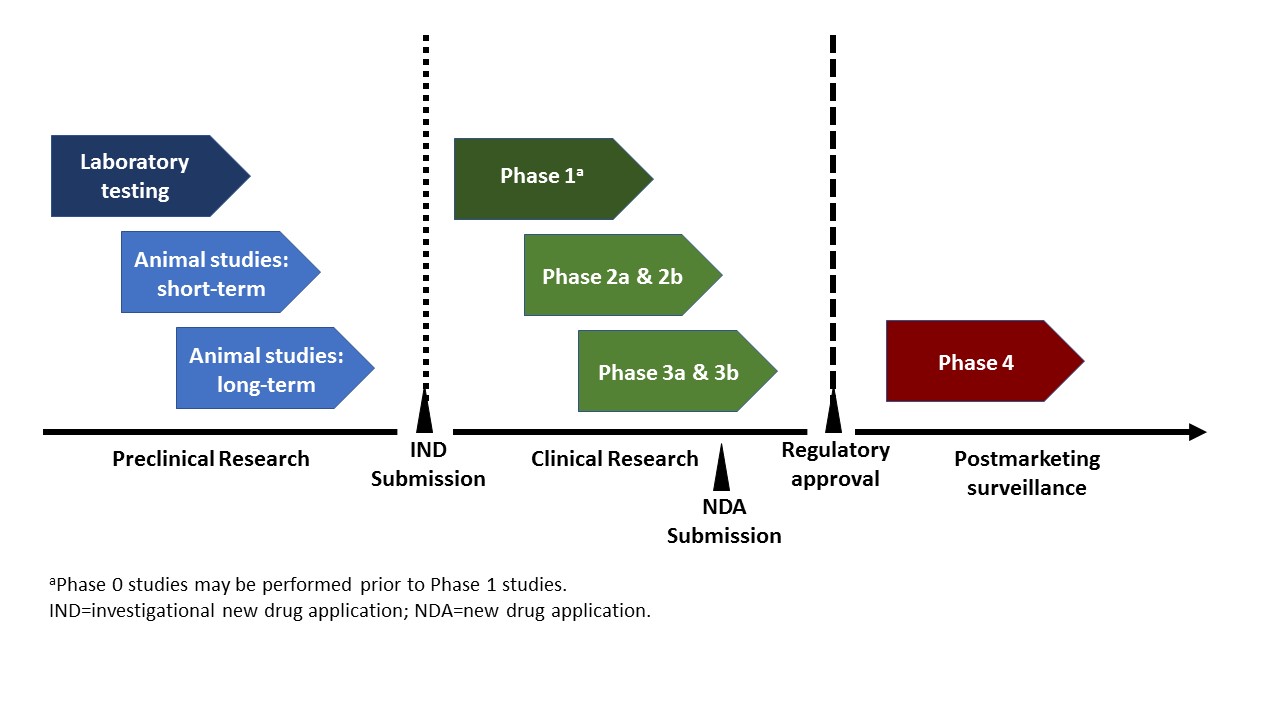
Clinical trials are typically conducted in four phases, and generally progress through the phases over many years (Figure 1 below).
- Phase 1: The first time an investigational treatment is tested in humans, phase 1 trials are designed to investigate safety, dosing, and metabolic, pharmacokinetic, and pharmacodynamic properties. Because they are first-in-human studies, they are often conducted on an in-patient basis, using a small number of subjects who may or may not have a disease, but more often than not, are healthy; however, for terminal conditions (eg, cancer), patients with advanced disease may be included because there are no better options. These trials are usually single-arm trials (see Clinical Trial Designs section below). A relatively new designation, called phase 0 or micro-dosing studies, has recently been introduced. These trials are designed for more rapid drug development, and are characterized by the administration of sub-therapeutic doses of the investigational product to a small number of subjects to assess pharmacokinetics only.
- Phase 2: These trials are conducted in a larger group of subjects who have the disease for which the investigational intervention is being developed. Phase 2A trials are specifically designed to assess dosing, while Phase 2B studies look at efficacy. These trials often have a control group, with patients randomly assigned to either the treatment or the control.
- Phase 3: The study population of these trials are larger and with the disease. These trials are conducted as randomized studies, and are generally required for regulatory approval. They are designed to test a treatment’s efficacy, monitor safety and side effects, and, if applicable, evaluate it against standard-of-care, which may be placebo or an active comparator. Because of the large number of patients needed, they are usually conducted at multiple sites and sometimes in multiple countries (for a large global study).
- Phase 4: After a drug has been approved, there is often additional information requested by health authorities regarding efficacy and safety, effects on quality of life, pharmacoeconomics, etc. These studies, termed post-marketing or post-approval studies, can be either observational or randomized, and may be conducted under real-world conditions or may be supervised as with earlier phase trials (eg, in-patient).
 Figure 1. Typical drug development plan.
Figure 1. Typical drug development plan.
{kind=link}
Clinical Trial Designs
Clinical trials can be designed in different ways depending on the clinical question being investigated.
- Randomized: This is what most people think of when they hear “clinical trial.” They are designed to compare interventions. Participants are randomly assigned to one of two or more groups that include the investigational intervention(s) and a comparator, which can be placebo or another treatment (ie, current standard of care).
- Single-arm: These trials test only a single intervention. Phase 1 trials are usually conducted as single-arm studies. A single-arm design may also be used if there are no alternative interventions or if during the randomized phase of a trial, the alternative was shown to be inferior, so only one treatment is administered during the long-term extension.
- Crossover: In this type of study, subjects are administered one treatment and then, after a prespecified period of time (and potentially a wash-out period), are switched to the other treatment, and those on the second treatment are switched to the first. This allows for each patient to serve as their own control, and is particularly useful for conditions for which it is difficult to recruit participants.
- Observational: These studies are utilized after a product has been approved, and follow subjects over time under real-world conditions (prospective), or look retrospectively at patient charts. Because these studies are performed in clinical practice, the patient populations and protocols are generally less restrictive than other trial designs. Whereas in other types of clinical trials, treatments are administered under strict supervision over adherence and adverse effects; because observational studies do not actively intervene, more realistic information about a given treatment can be derived.
Clinical trials can be either blinded or open-label.
- Blinded: The purpose of blinding is to protect against bias. There are different degrees of blinding. In single-blind trials, the observer/researcher, but not the subject, knows which intervention is being administered to whom. In double-blind trials, neither the observer/researcher nor the subject knows who is receiving which intervention). In triple-blind trials, the observer/researcher, subject, and person analyzing the results are all ignorant on who received the investigational intervention.
- Open-label: In these trials, everyone involved knows which treatment is being administered to whom. These trials may still be randomized or they may be uncontrolled, with all participants receiving the same treatment (single-arm). They may be conducted as extensions of randomized, blinded trials, or a trial may be open-label if the difference between interventions is obvious (eg, oral vs injection).
|
Participants in clinical trials should only be referred to as “patients” if they have a disease. |
Clinical Trials Good Practices
All clinical trials are mandated by the US Food and Drug Administration (FDA) to be listed on the US National Institutes of Health (NIH) website, clinicaltrials.gov, which is an international registry and results database of publicly and privately supported studies that enroll human participants. Phase 1 studies are exempt. Study registration is required to be posted on the site no later than 21 days after the first patient is enrolled, and basic results are required to be posted no later than 1 year after the primary completion date. The European Union has a similar registry.
The ethical conduct of clinical trials is of upmost importance, and to that end, the International Conference on Harmonisation (ICH) developed unified standards for the conduct, recording, and reporting of clinical trials. Independent institutional review board (IRB) approval of the protocol, amendments, and other documentation is required before a study can begin, and continues as the study progresses. Some components that ensure patient safety include mandating informed consent of all participants, establishment of safety monitoring boards, and appropriately designing the trial with enough power and in a manner that answers the clinical question.
Publication of Clinical Trial Data
Clinical studies provide an enhanced understanding of a disease state and/or demonstrate the safety and/or efficacy of a potentially valuable new therapeutic modality. Therefore, clinical studies have the potential to benefit people other than those directly involved in the studies. But, this can only happen if the results are made public, and that is where publications play a critical role.
Whether the results are positive (investigational product showed superiority to control) or negative (investigational product did not show superiority to control), the results of every clinical trial should be published. Knowing what does not work is equally important to knowing what does. Although international regulations differ, the updated Good Publication Practice (GPP3) guidelines, published in the Annals of Internal Medicine and sponsored by the International Society for Medical Publication Professionals (ISMPP), recommends the submission of manuscripts within 12 months of study completion for licensed products and of product approval for investigational products (Battisti 2015).
Because each clinical trial format is designed to answer a specific type of clinical question, it is important to accurately and completely describe the methods when writing up the results of a study for publication. The validity of the results and conclusions will be judged by the appropriateness of the methods used. Critical components include the study design, subjects, outcome measures, and statistics used for analyzing the outcome measures. In addition, the rationale and limitations of the methodology should be explained in the discussion.
The CONSORT Statement was developed by a group of medical journal editors, clinical trialists, epidemiologists, and methodologists to standardize and improve the reporting of randomized clinical trials. Currently, 585 journals endorse CONSORT, and require the submission of the CONSORT checklist along with the manuscript.
As publication professionals, we must understand the nuances of each type of study, so that we can effectively assist in the dissemination of the results to the medical community at large, where the information can ultimately help patients.
Reference
Battisti WP, Wager E, Baltzer L, Bridges D, Cairns A, Carswell CI, Citrome L, Gurr JA, Mooney LA, Moore BJ, Peña T, Sanes-Miller CH, Veitch K, Woolley KL, Yarker YE; International Society for Medical Publication Professionals. Good Publication Practice for Communicating Company-Sponsored Medical Research: GPP3. Ann Intern Med. 2015 Sep 15;163(6):461-4.