
Richard White, MA, PhD, Oxford PharmaGenesis Ltd, Oxford, UK; Gemma Carter, PhD, Oxford PharmaGenesis Ltd, Oxford, UK; Jacob Willett, MPH, Oxford PharmaGenesis Inc., Newtown, PA, USA
This article is part of the Medical Publications 101 article series, which serves as an introduction to various topics that are relevant to medical publication professionals.
What Is RWE and Why Is Everyone Talking About It?
Real-World Evidence (RWE), according to the International Society for Pharmacoeconomics and Outcomes Research (ISPOR), comprises “Data used for decision-making that are not collected in conventional randomized controlled trials (RCTs).” 1 RWE is not new; collection of RWE has been mandated for the pharmaceutical industry for many years in post-launch safety studies/pharmacovigilance, and in registries for rare diseases. What is new is the application of RWE to show the unmet need for a new intervention pre-launch, and to demonstrate the effectiveness of a new intervention post-launch.
The need to generate evidence of value throughout a product life cycle has been driven by the demands of payers, clinicians – and increasingly, regulators.
- The Food and Drug Administration (FDA) has already released draft guidance on the use of RWE for the evaluation of medical devices,2 and has stated that it is important to “…consider the possibilities of using so-called ‘real world’ data as an important tool in evaluating not only the safety of medications but also their effectiveness…” 3 FDA will begin consultation in 2018 on use of RWE in decision-making for issues such as label expansion, new indications, and identification of target patient populations.
- The European Medicines Agency (EMA) is developing its Adaptive Pathways approach to licensing new interventions in areas of high medical need in which it is difficult to collect data via traditional routes.4 This approach involves:
- conditional approval or approval based on early data (using surrogate endpoints) considered predictive of important clinical outcomes
- gathering RWE to supplement clinical trial data and confirm the benefit–risk profile of the intervention
In Europe, the GETREAL initiative has brought together pharmaceutical companies, academia, reimbursement agencies, regulators, and patient organizations to “…show how robust new methods for RWE collection and synthesis could be adopted earlier in pharmaceutical research and the healthcare decision-making process.” 5 Several pharmaceutical companies have responded to these trends by publishing their own “position papers” on the use of RWE.6,7
While the debate so far has focused on the generation and application of RWE, both of these rely on the effective communication of RWE – and this is where the role of the medical publications professional will be important.
What Are the Major Approaches for Gathering RWE?
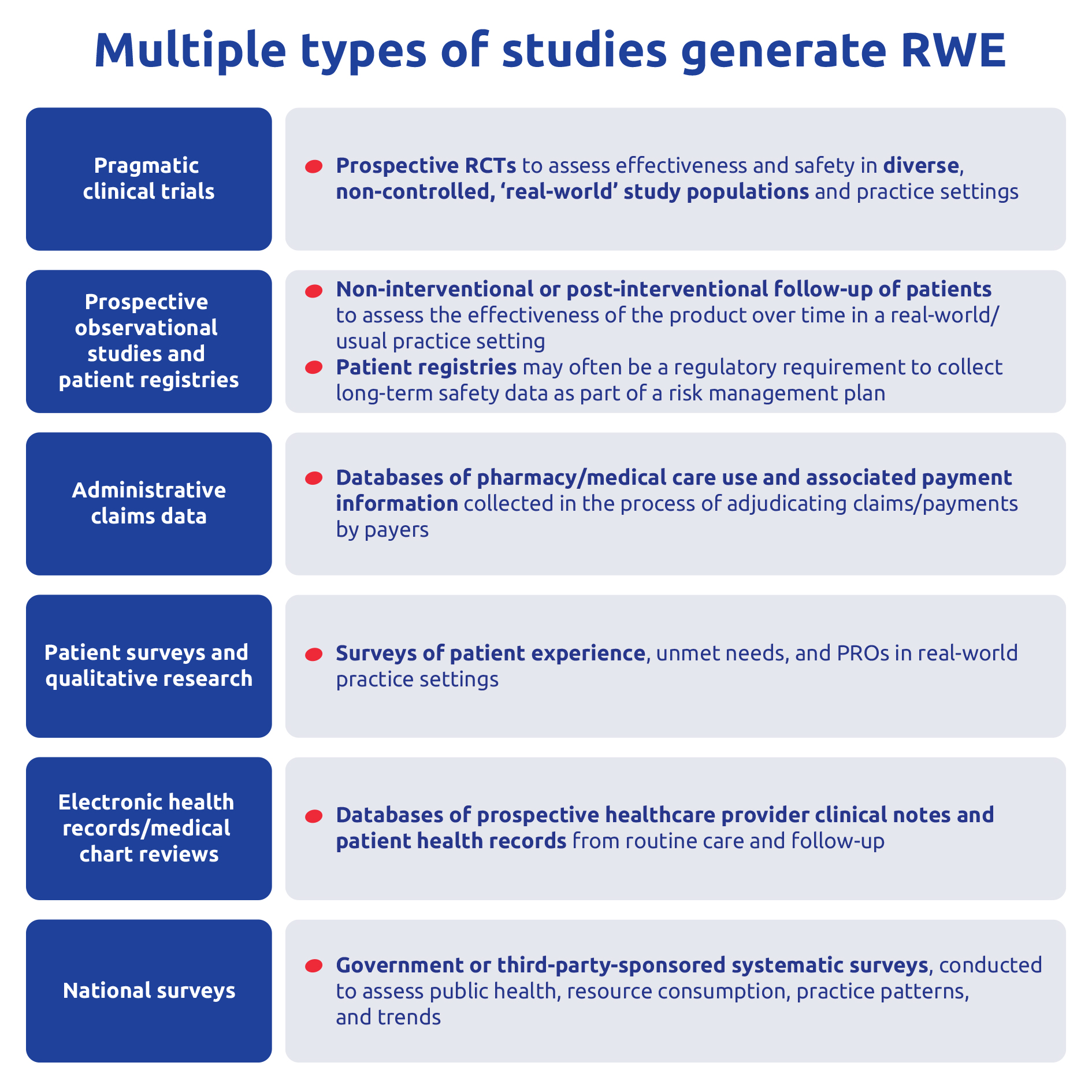
The term RWE is being widely applied to include what were previously called “observational” or “non-interventional” studies (ie, studies in which the researcher has no control over the medical management of the patient beyond observing the outcomes). Many sources of RWE now exist, and a helpful overview of the different data sources and their potential applications is provided by the GETREAL RWE Navigator8 and by other organizations and initiatives, such as the Agency for Healthcare Research and Quality (AHRQ), ISPOR, Patient-Centered Outcomes Research Institute (PCORI), and STRengthening Analytical Thinking for Observational Studies (STRATOS). The major sources of RWE are summarized in Figure 1 below.
{kind=link}

Figure 1. The major sources of RWE.
Summarized based on information at https://rwe-navigator.eu.
Traditional RWE methodologies can be either prospective or retrospective.
- Prospective – the data are collected after the study is designed and initiated; the most common approach is a patient registry or prospective observational study.
- Retrospective – the data have already been collected, and the study is designed to analyze these data; this methodology is often applied to administrative claims, survey data, and health records.
Pragmatic clinical trials are a growing area and are at the boundary between RCTs and RWE. An example is the Salford Lung Study in the UK, which randomized a real-world patient population (ie, including many co-morbidities that would lead to exclusion from a traditional RCT) to a new chronic obstructive pulmonary disease intervention or to current standard of care, and with data collected prospectively through essentially real-world methods (ie, electronic health records).9
RWE is a rapidly evolving field, and traditional approaches are being augmented by data from emerging sources, such as health-monitoring devices, health apps, and social media (eg, Facebook posts, Twitter tweets). These pose several new challenges for analysis and interpretation as follows:
- Data contributed via these sources are not usually linked to a diagnosis by a clinician, leading to uncertainty over which disease the data refer to (eg, for a gastrointestinal disorder, the diagnosis could be irritable bowel syndrome, or irritable bowel syndrome with constipation, or chronic constipation, or irritable bowel disease, or Crohn’s disease…).
- Data contributed via these sources come from a self-selected population, which fundamentally limits the generalizability of the results.
- Social media, in particular, provides unstructured data – messages, videos, photos, and audio files – that cannot directly be categorized under a particular theme or endpoint.
What Insights Can RWE Provide Beyond Traditional RCTs?
RCTs are still widely held to be the “gold standard” for evidence-based medicine, but the strengths of a highly controlled interventional study design in generating robust comparative data can be weaknesses when drawing conclusions for everyday practice. For example, more than three-quarters of RCTs exclude patients with comorbidities, even though most patients in real-world practice have concomitant chronic conditions.10 RWE can, therefore, provide important insights that are complementary to those provided by RCTs:
- Assessment of effectiveness in a real-world setting
- Diverse population reflective of real-world physician/patient characteristics (eg, guideline use, non-adherence, off-label use, comorbidities)
- Comparative evidence against multiple realistic comparators
- Comparison ideally with current standard treatment (which differs by patient segment and country), not placebo
- Broader range of real-world outcomes
- Patient experience, patient-reported outcomes (PRO), healthcare resource utilization, costs
- Improved understanding of benefit–risk profile
- Assess long-term clinical benefits and rare adverse events
- Locally relevant data
- Data can be specific to a region or country, whereas most RCTs are multinational
Generating RWE early in the product development process (ie, early in phase 2) can also help to develop RCTs that are more representative of clinical practice, by validating outcomes and informing the choice of patient population and comparator for subsequent phase 3 RCTs.
What Are the External Challenges to Acceptance for RWE, and How Do We Overcome Them?
Despite the increasing demand for RWE, most decision-makers still consider RWE to be a less robust source of evidence than RCTs. A recent editorial addressed key reasons why RWE is not widely accepted.11 The external challenges and potential solutions are covered briefly in Table 1 below.
| What’s the issue? (click on links below for further explanation) |
What’s the question that we need to answer? | How do we address this challenge? |
| Lack of randomization and risk of bias in RWE | “If you haven’t randomized, how do you know that you are comparing apples with apples?” | Transparency in methodology – apply and explain the methods used to minimize bias and confounding factors |
| Representativeness of results | “Did you use the best RWE data source to ensure that your study is representative – or just the cheapest/quickest/easiest?” | Transparency in data sources – conduct and publish a systematic assessment to show that your RWE study used the most appropriate sources |
| Multiplicity of studies | “How can we be sure you didn’t do lots of RWE studies and publish only the one that gave the results you wanted?” | Transparency in strategy – create internal policies that commit to posting protocols and publishing, regardless of the direction of the results |
| Contradiction of studies | “If your RWE study gives the opposite result to a competitor’s study, how can we tell which is more robust?” | Transparency in reporting – utilize best practice guidelines on communicating RWE studies (eg, STROBE, MOOSE, AHRQ*) |
Table 1. The major external challenges to acceptance of RWE.11
*AHRQ: Agency for Healthcare Research and Quality; MOOSE: Meta-analysis Of Observational Studies in Epidemiology; STROBE: Strengthening the Reporting of Observational Studies in Epidemiology
© Oxford PharmaGenesis 2017
What Are the Internal Challenges for RWE Study Publications?
It is not only external audiences who may question the fundamental robustness and validity of RWE studies. Similar challenges can also come from internal functions (eg, clinical development, medical affairs, statistics, regulatory, legal) who are accustomed to the rigor of RCTs. Transparent communication, education, and training on the fundamentals of RWE are important, but the medical publications professional must also be ready to overcome several operational issues specific to RWE studies (Table 2 below).
| What’s the issue? | Why is RWE different from RCTs? | How can medical publication professionals help? |
| RWE data set maturation and robustness of analysis | Whereas timing of data availability for RCTs is highly predictable, it is often the case for RWE that when analysis is completed, the data set turns out not to be sufficiently mature (ie, contains insufficient data) to draw meaningful conclusions. | Conduct publication planning “at risk” for most RWE studies, and establish contingencies (eg, submission to a “fall-back” conference later in the year) |
| Flexibility in analysis timing | RWE study concept sheets (or registry data request forms) are less rigid than RCT protocols; hence, authors and journal peer reviewers are more likely to request exploratory, “what if…?” analyses. | Encourage the wider RWE study team to pre-plan analyses as far as possible, and stick to them; ClinicalTrials.gov has been used to post RWE study plans.12
|
| Flexibility in analysis scope | Whereas RCT results are defined at database lock, RWE databases and registries grow over time – hence, repeated analyses may give increasingly more robust results. | Recommend that authors resist the temptation to re-analyze results during publication development, and plan in advance for update publications (eg, 6-month and 12-month follow-up analyses). |
| Target journal selection | Journals may not be interested in country/region-specific RWE, may lack peer reviewers who can review RWE manuscripts properly, or may simply not accept industry-sponsored RWE studies. | Go beyond usual approaches to journal shortlisting; map historical journal publication patterns, and speak with journal publishers/editors to define journal suitability for RWE studies.13 |
Table 2. Differences between RCTs and RWE that create challenges for publication practice
© Oxford PharmaGenesis 2017
What Does the Future Hold for RWE?
The future of RWE is best summarized with reference to a concept that is familiar in the area of “big data” – the “4 Vs”:
- Volume
- More and more RWE will be generated, driven by increasing demand from regulators, payers, and physicians pre- and post-launch. Medical publication professionals will need to adapt to a world in which publication plans increasingly comprise RWE rather than RCTs.
- Variety
- The current favored sources of RWE are rapidly being augmented by emerging sources, such as health-monitoring devices, health apps, and social media. Medical publication professionals will need to consider how to handle these important but unfamiliar sources of RWE. A particular challenge will be communicating and publishing insights from unstructured data (eg, social media posts), and studies utilizing multiple linked data sources.
- Velocity
- Some emerging sources of RWE will provide real-time data with potentially immediate clinical relevance. While processing these data and making treatment decisions based on the observed trends may be outside the realm of the medical publications professional, new approaches to publication and communication will be necessary to show the impact of such high-velocity data.
- Veracity
- As computing power increases and data analytics methodologies become more sophisticated, RWE studies will increasingly involve larger data sets (aggregating and linking multiple individual data sources) and be able to provide more robust and reliable insights to guide clinical decision-making. Medical publication professionals will need to keep themselves informed on advances in this area in order to be effective in planning and executing publications from RWE studies.
Many of the challenges posed by RWE are not directly related to communication. However, with effective collaboration and transparent communication, medical publication professionals can help to break down the remaining skepticism towards RWE. This, in turn, will harness the power of RWE for the all-important “5th V” – demonstrating the value of new interventions for the patients who most need them.
References
- Garrison LP Jr, Neumann PJ, Ericsson P et al. Using real-world data for coverage and payment decisions: the ISPOR Real-World Data Task Force report. Value Health 2007;10:326–35.
- US Food and Drug Administration. Use of real-world evidence to support regulatory decision-making for medical devices. Available from: https://www.fda.gov/downloads/medicaldevices/deviceregulationandguidance/guidancedocuments/ucm513027.pdf. Accessed 23 March 2017.
- US Food and Drug Administration. PDUFA reauthorization performance goals and procedures: fiscal years 2018 through 2022. Available from: www.fda.gov/downloads/forindustry/userfees/prescriptiondruguserfee/ucm511438.pdf. Accessed 23 March 2017
- European Medicines Agency. Adaptive pathways. Available from: http://www.ema.europa.eu/ema/index.jsp?curl=pages/regulation/general/general_content_000601.jsp. Accessed 23 March 2017.
- Innovative Medicines Initiative. Get real. Available from: https://www.imi.europa.eu/content/getreal. Accessed 23 March 2017.
- Berger ML, Lipset C, Gutteridge A et al. Optimizing the leveraging of real-world data to improve the development and use of medicines. Value Health 2015;18:127–130.
- Galson S, Simon G. Real-world evidence to guide approval and use of new treatments. National Academy of Medicine, Washington, DC 2015. Available from: https://nam.edu/wp-content/uploads/2016/10/Real-World-Evidence-to-Guide-the-Approval-and-Use-of-New-Treatments.pdf. Accessed 23 March 2017.
- Innovative Medicines Initiative. RWE Navigator. Available from: https://www.imi-getreal.eu/Publications/RWE-Navigator. Accessed 23 March 2017.
- Vestbo J, Leather D, Diar Bakerly N et al. Effectiveness of fluticasone furoate–vilanterol for COPD in clinical practice. Available from: http://www.nejm.org/doi/full/10.1056/NEJMoa1608033. Accessed 23 March 2017.
- Buffel de Vaure C, Dechartres A, Battin C et al. Exclusion of patients with concomitant chronic conditions in ongoing randomised controlled trials targeting 10 common chronic conditions and registered at ClinicalTrials.gov: a systematic review of registration details. BMJ Open 2016;6:e012265.
- White R. Building trust in real-world evidence and comparative effectiveness research: the need for transparency. J Comp Eff Res 2016;6:5–7.
- ClinicalTrials.gov. Real-world effectiveness and cost-effectiveness of Qvar versus FP, a US study (USQvarAsthma). Available from: https://clinicaltrials.gov/ct2/show/NCT01287351. Accessed 23 March 2017.
- Schmidt L, Elvelin L, Farrow P et al. A systematic approach to journal selection with the aim of improving acceptance rates of real-world evidence publications [poster]. Presented at the 2017 European Meeting of the International Society for Medical Publication Professionals (ISMPP), 17–18 January 2017, London, UK.
Discover more from the Map Newsletter
Subscribe to get the latest posts sent to your email.